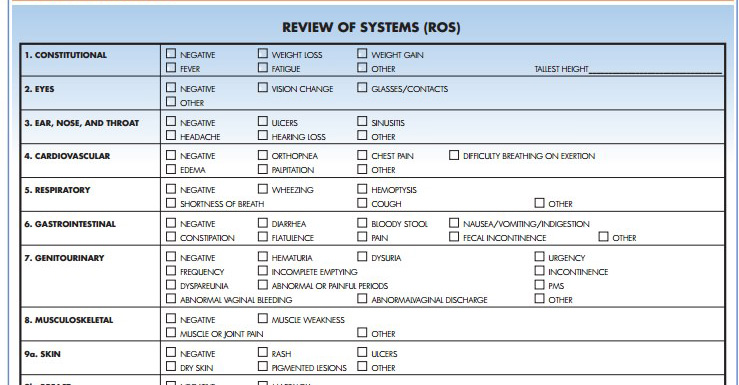
ROS – Review of Systems
The following list shows the content of a systems review that can be incorporated into the patient history.
General/ Constitutional
Skin
Head
EENT
Neck
Breast
Respiratory
Cardiovascular
Gastrointestinal
Genitourinary
Female
Male
HIV Status
Endocrine
Musculoskeletal
Neurologic
Hematologic
Psychiatric
General
- Weight – average, recent changes, minimum, maximum
- Weakness, fatigue, fever
- Sweats, chills
- Anorexia
- Insomnia (can’t sleep)
- Hypersomnolence (sleep all the time)
Skin
- Lesions, lumps, growths, sores
- Moles, change in color/pigmentation, eruptions/rashes
- Pruritus (itching)
- Dryness, excessive sweating
- Easy bruising
- Changes in nails/hair
- Birthmarks
- Change in temperature
Head
- headache
- head injury
- change in size
- deformity
- dizziness
- syncope (lightheaded)
- vertigo (spinning)
EENT
- Eyes: use of glasses/contacts, pain, diplopia (double vision), glaucoma, cataracts, itching, spots, photophobia, color blindness, night blindness, blurry vision, ptosis (droopy eyelids), halos (rings around lights), scotomata (blind spot), redness, tearing, discharge (color, consistency), use of eye drops, last eye exam
- Ears: pain, hearing loss, deafness, discharge (color, consistency, bloody), infections, tinnitus (ringing), vertigo, pruritus (itching), use of hearing aid
- Nose/Sinuses: rhinorrhea (runny nose), nausea, vomiting, hematemesis (vomiting stuffiness, discharge (color, consistency), pruritus (itching), epistaxis (nose bleeds) pain over sinuses, hay fever, frequent colds
- Throat/Mouth: sores, lesions, condition of teeth and gums, dental caries, loss of teeth, dentures, bleeding, sore throat, hoarseness, change in taste, bad taste, malodorous breath, dry mouth, last dental exam
Neck
- Pain, swelling
- Limits in range of motion or stiffness
- Lumps, swollen lymph nodes
- “Swollen glands”
Breast
- Lumps, pain, swelling
- Nipple discharge
- Use of self-exam, last mammogram
Respiratory
- Cough, sputum (color, quantity), hemoptysis (blood from lungs/bronchus)
- Wheezing, asthma, emphysema, bronchitis, pneumonia, tuberculosis, pleurisy
- Shortness of breath
- Last chest x-ray
Cardiovascular
- History of heart disease
- Chest pain (exertional/nonexertional, associated symptoms)
- Orthopnea (discomfort breathing by lying flat)
- PND (Paroxysmal Nocturnal Dyspnea)
- Dyspnea on exertion (shortness of breath)
- Edema, cyanosis (blue skin)
- Palpitations (irregular heartbeats)
- Loss of consciousness
- Hypertension, heart murmur
- Claudication (limping/calf muscle weakness)
- Thrombophlebitis (inflamed veins)
- Varicosities (dilated veins)
- Raynaud’s Phenomenon (bilateral cyanosis of digits)
- Rheumatic Fever
Gastrointestinal
- Change in appetite
- Abdominal pain, difficulty/pain with swallowing Heartburn, indigestion, bloating, belching, blood), jaundice
- Food intolerance
- Frequency of bowel movements
- Change in bowel habits (frequency, consistency, caliber, constipation, diarrhea), melena (dark colored stools), hematochezia (bloody stools), clay-colored stools, mucus (passing mucus)
- Excessive belching or passing of gas
- Incontinence (inability to prevent discharge)
- Hemorrhoids, rectal itching/burning
- Rectal discharge/pain
- Laxative use
- Hepatitis, gallbladder disease
Genitourinary
- Frequency of urination
- Dysuria (difficulty pain urination)
- Hematuria (blood in urine)
- Change in color of urine
- Polyuria (excess urine)
- Nocturia (pee a lot at night)
- Oliguria (not much urine), anuria (no urine)
- Flank suprapubic pain
- Retention (can’t fully void)
- Urgency (desire to void)
- Hesitancy involuntary delay)
- Incontinence, change in force of stream
- Dribbling, passage of air/stone
- Enuresis (leakage of urine)
- Past infections
Female
- Menstrual history (onset cycle duration, amount of flow, change in cycle)
- LMP amenorrhea (loss of cycle), menorrhagia (excessive menses), metrorhagia (irregular menses), associated pain or PMS symptoms
- Contraceptive history • Previous pregnancies deliveries, abortions, complications, outcomes) Exposure to DES (diethylstilbestrol) Vaginal discharge, pruritus, abscess, sores, lesions, infections, STI’S, PID (Pelvic Inflammatory Disease), RPR status (Rapid Plasma Reagin test – syphilis). HIV status,
- Previous PAPs
- Premenstrual symptoms
- Problem with intercourse (pain, satisfaction, libido), sexual orientation number of partners
- Age at menopause
- Postmenopausal bleeding • Menopausal symptoms (hot flashes, mood swings, changes in vaginal lubrication)
Male
- Hemias
- Penile discharge
- Sores
- Testicular pain or lumps
- STI’S
- RPR (Rapid Plasma Reagin test – syphilis)
HIV status
- Sexual orientation number of partners
- Problems with intercourse (impotence satisfaction, sex drive)
- Contraceptive use
Endocrine
- Goiter, exophthalmos (eyeballs protrude)
- Hot/cold intolerance, constipation/diarrhea
- Tremor, excessive sweating
- Palpitations, change in voice
- Skin changes, hair distribution
- Secondary sex characteristics
- Changes in body contour or weight
- Changes in hat glove/shoe size
- Polyuria (increase urine), polydipsia (increase thirst). polyphagia (increase eating)
- Striae (stretch marks)
- Acne, pigmentation
- Infertility, diabetes, thyroid disorders
Musculoskeletal
- Pain in an extremity, joint pain
- Swelling, redness, stiffness, deformity, warmth
- Limited range of motion,
- Crepitation (cracking joints) – note location of each joint involved
- History of arthritis, muscle pain, gout, backache, neck pain, significant trauma
Neurologic
- Syncope, dizziness, seizures, vertigo
- Ataxia (uncoordinated movements), limp
- Frequent falls, tremor involuntary movement
- Weakness, loss of muscle mass, paralysis
- Clumsiness, pain
- Numbness, paresthesia (abnormal sensation, burning, tickling), hyperesthesia (abnormal acuteness to touch), dysarthria (speech change)
- Changing in handwriting
- Incontinence (bowel or urine)
Hematologic
- Anemia, easy bruising
- Past transfusions and any reactions to them
- IV drug use, enlarged lymph nodes
- Hemoglobinopathies (abnormal hemoglobins e.g., sickle cell anemia)
Psychiatric
- Nervousness, anxiety, mood swings, depression, crying spells, panic attacks
- Change in memory, early awakening problems sleeping, loss of energy
- Change in libido, suicidal thoughts
- Change in appetite, binge eating, purging
- Excessive exercising
- Paranoia, hallucinations, disturbing thoughts

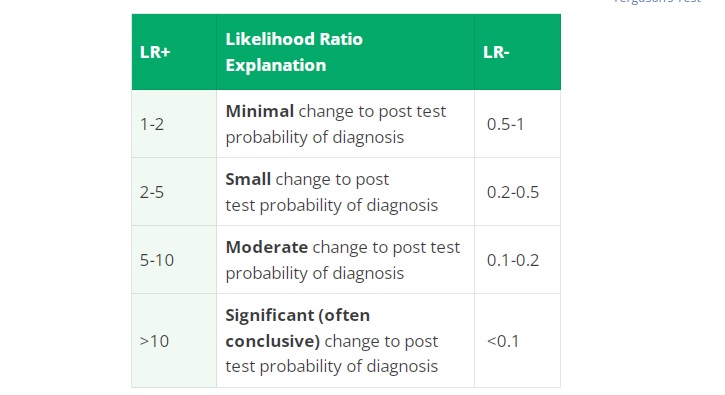
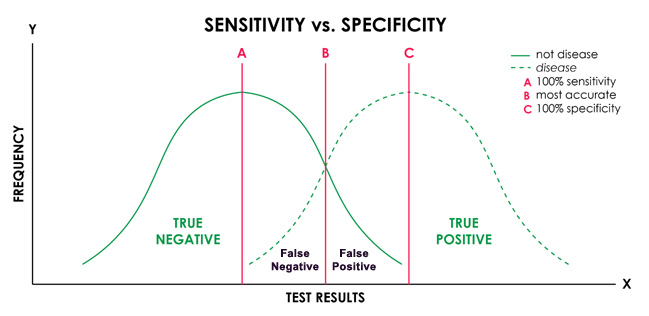
 Special Tests are orthopedic diagnostic tests that help identify the nature of musculoskeletal conditions. These special tests are used in creating a proper treatment plan or therapy for a patient’s injury or condition.
Special Tests are orthopedic diagnostic tests that help identify the nature of musculoskeletal conditions. These special tests are used in creating a proper treatment plan or therapy for a patient’s injury or condition.